A recent Supreme Court decision has ignited a fervent national debate, marking a significant development in the ongoing discourse surrounding state authority over healthcare funding and the future of reproductive services. The 6-3 ruling in a case stemming from South Carolina’s efforts to exclude Planned Parenthood from its Medicaid program has far-reaching implications, potentially reshaping the landscape of public health funding across the United States.
The core of the Supreme Court’s decision centers on whether patients can challenge a state’s decision to remove a healthcare provider, specifically Planned Parenthood, from its Medicaid program. The Court sided with South Carolina, asserting that patients do not possess the standing to bring such lawsuits. This ruling effectively upholds South Carolina’s policy, which aims to prohibit the use of taxpayer funds for abortions, thereby empowering states with greater autonomy in determining which providers can participate in their Medicaid programs.
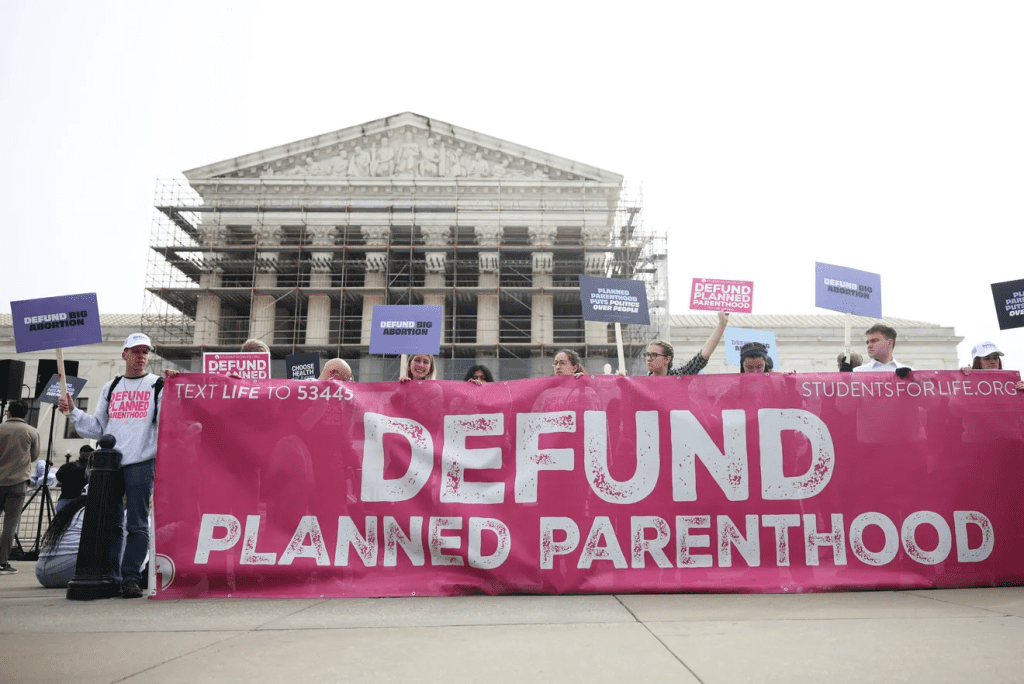
This legal development is viewed by its proponents as a victory for fiscal conservatism and the pro-life movement. They argue that the decision ensures taxpayer money is not allocated to organizations that perform abortions, aligning with the principles of those who believe in the sanctity of life. Data cited indicates that Planned Parenthood conducted nearly 400,000 abortions in 2022, representing over 60% of all reported abortions in the U.S. From this perspective, the ruling is a crucial step towards redirecting public funds away from abortion services and towards other healthcare providers. The argument is often made that numerous other governmental and non-governmental entities are available to provide comprehensive healthcare services to women, thus negating the necessity of Planned Parenthood’s participation in state Medicaid programs.
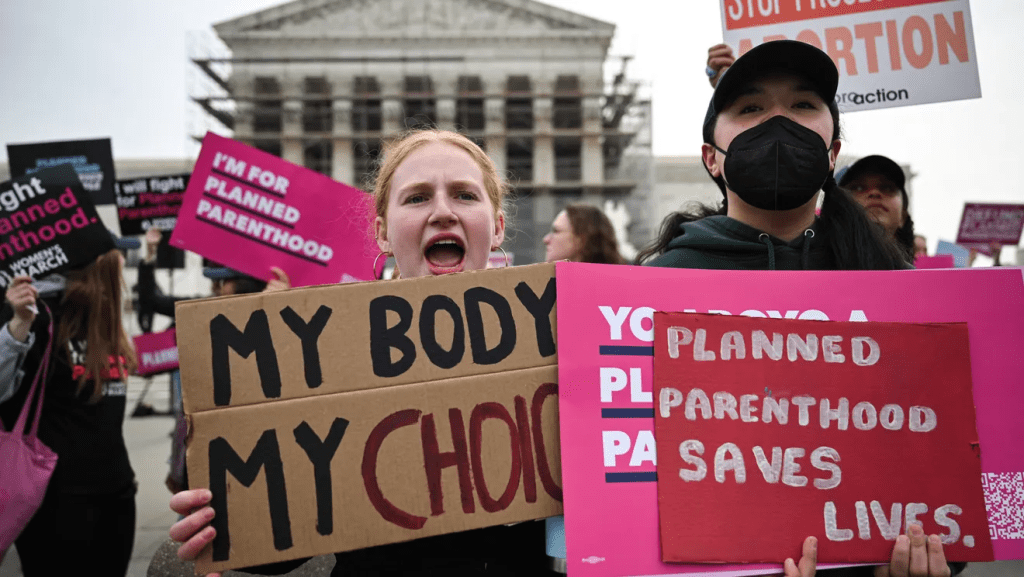
Conversely, critics of the ruling contend that it represents a significant setback for women’s healthcare access, particularly for low-income individuals who rely on Medicaid. They argue that restricting Planned Parenthood’s access to Medicaid funding, which historically has constituted a substantial portion of its budget (approximately 40%, or over $500 billion annually from Medicaid and other government sources), will severely limit the availability of a wide range of essential services. These services, beyond abortion, include contraception, cancer screenings, and STI testing and treatment. Opponents highlight that while abortion services are a part of Planned Parenthood’s offerings, they represent a minority of the total services provided, and the organization is a major provider of primary and preventive care for many underserved communities. The concern is that this decision could disproportionately affect vulnerable populations by reducing their options for affordable and accessible healthcare, potentially leading to adverse health outcomes.
The ruling has sparked renewed calls for other states to follow South Carolina’s lead, potentially leading to a nationwide trend of defunding Planned Parenthood through Medicaid exclusions. This prospect raises profound questions about the future of reproductive rights and healthcare equity. As states gain more power to shape their Medicaid programs, the variations in healthcare access across different states could become even more pronounced, creating a fragmented system where access to critical services depends heavily on geographical location.
Ultimately, the Supreme Court’s decision is not merely a legal pronouncement; it is a catalyst for an intensified national dialogue on federal versus state power, the allocation of public funds, and the fundamental right to healthcare. Its long-term impact on Planned Parenthood’s operations, women’s health outcomes, and the broader healthcare landscape remains to be seen, but its immediate effect is to further polarize an already deeply divided issue in American society.